Minimally
invasive surgery
My
primary research interests are in incorporating haptic
interaction and image
guidance in
computer-assisted surgery and therapy, which mainly involve the areas
of medical robotics (including haptics, teleoperation and controls) and
medical image processing. My application of interest has so far been
minimally invasive surgery (MIS). In minimally invasive
(endoscopic/laparoscopic) surgery, thin instruments are inserted into
the body cavity through small incisions rather than making a large
incision as in open surgery.
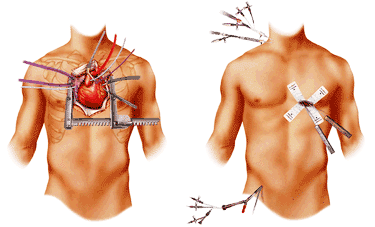
Open
surgery (left), minimally invasive surgery (right).
[Picture from
Anova Heart and Vascular Institute website]
Conventional
versus robot-assisted MIS
Although
MIS significantly reduces patient morbidity and length of hospital stay
because of the small incision size, it has inherent drawbacks to the
surgeon in terms of motor functioning and sensory capabilities. These
include significantly degraded haptic feedback about instrument/tissue
interactions, degraded visual feedback, and reduced dexterity and fine
manipulation capability. Image-guided MIS attempts to use medical
images (ultrasound, CT, etc.) to automate tasks through guiding
surgical instruments to desired positions in the patient, generally
either through incorporation with the control algorithm for a surgical
robot or through virtual reality (e.g., image overlays on the
endoscopic camera view in MIS) used to inform the surgeon. I am
interested in the use of robotic and mechatronic systems, haptic
interaction and image
guidance for tackling the motor/sensory limitations that exist in MIS
(or similar medical and biomedical applications).
A
teleoperation system with haptic interaction
With a
limited maneuverability of surgical instruments and restricted camera
vision experienced in MIS, haptic feedback to the surgeon can be very
helpful and make these kind of procedures more natural and less
cumbersome. Studies have shown that the presence of haptic
interaction in master-slave teleoperation, whereby a user operates from
and receives force feedback via a master interface while a slave robot
mimics the user’s hand maneuvers, enables significantly better control
over tool-tissue interaction. The lack of haptic interaction has been
identified as a major drawback of the current robotic-assisted surgical
system, and a satisfactory solution has yet to be developed.
My
research pertained to devices and methods required for restoring haptic
feedback in robot-assisted MIS. In terms of devices, I
augmented a 3-DOF PHANToM haptic device with two additional degrees of
freedom to form a surgeon-robot interface with full force reflection
capabilities. I also designed a slave surgical end-effector
with force sensing capabilities in all of the five degrees of freedom
present in laparoscopic surgery.
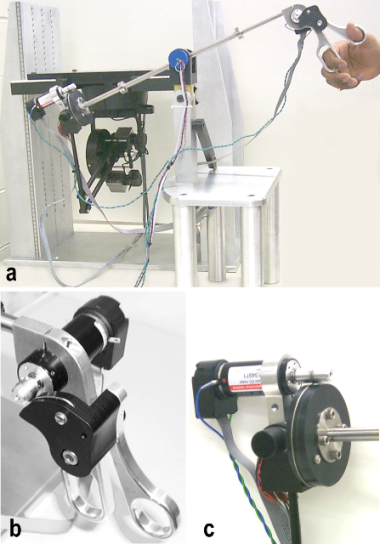
Left:
(a) Haptic user interface for endoscopic interventions. Mechanisms for
force reflection in the finger loops (b) and the roll mechanism (c).
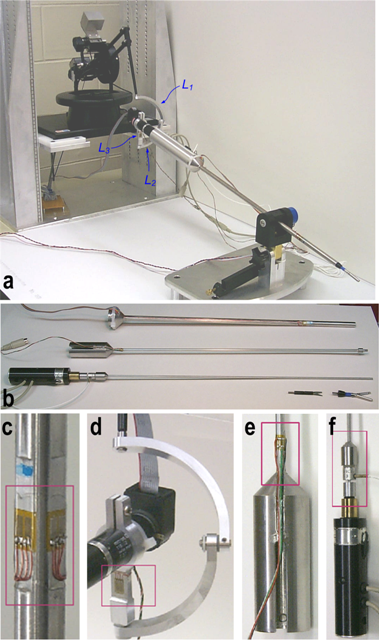
Right: (a)
Sensorized slave robot including the end-effector, the wrist, the twist
motor, and the tip actuation assembly. (b) Details of the tip actuation
assembly: the three tubes and two different detachable tips. (c) Gauges
to measure bending moments. (d) Gauges to measure axial forces. (e) A
gauge to measure torsional moment. (f) A load cell to find tip forces.
Back
to Research